Clinical Reasoning AR
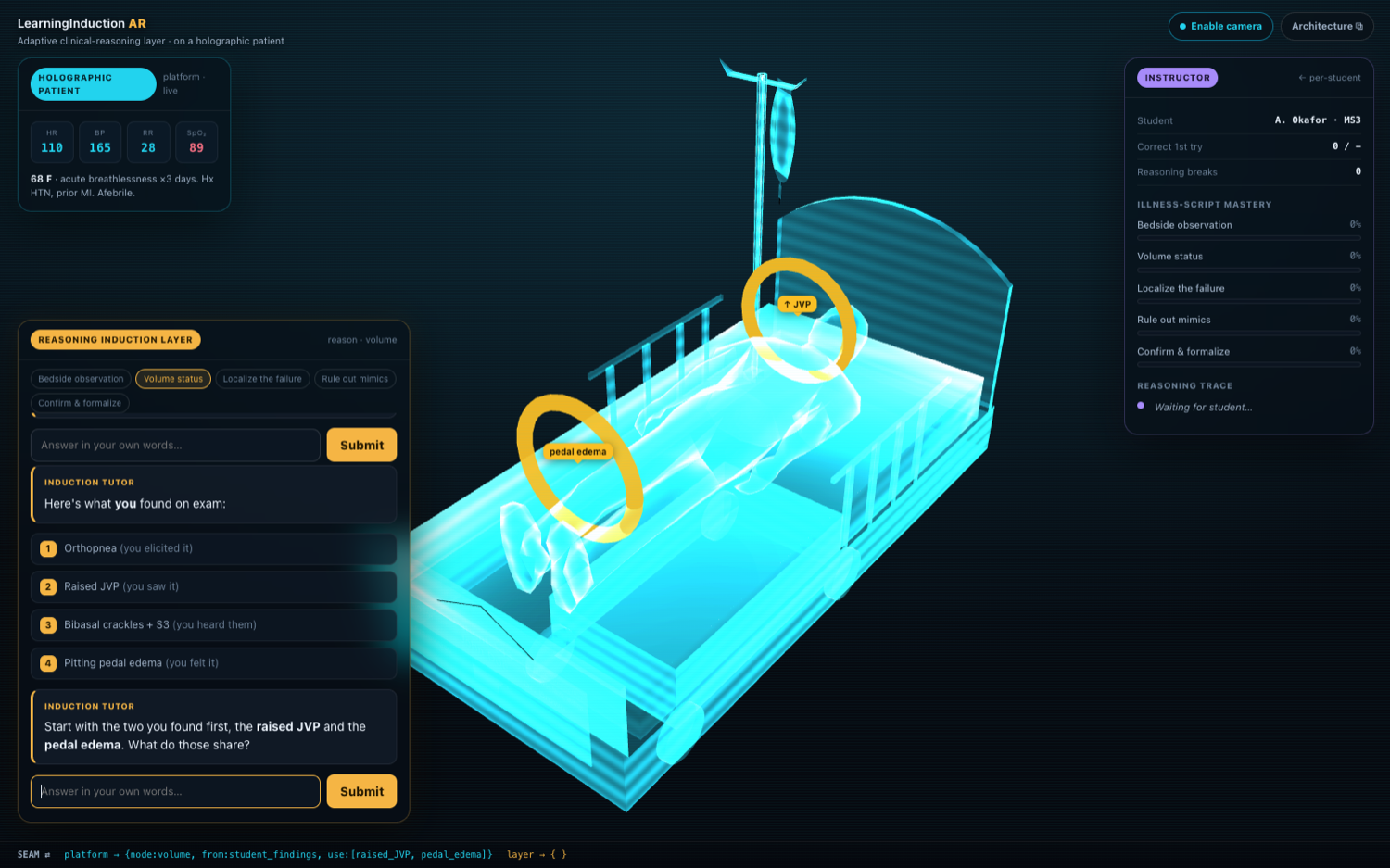
Third-year medical students know the theory but freeze at the bedside. I designed an adaptive tutor that makes them discover the clinical reasoning themselves, on a holographic patient, so the knowledge actually transfers. It’s built to ride on top of an XR clinical simulation platform.
The transfer gap isn’t only a knowledge gap, it’s a reasoning gap. So instead of explaining more, the tutor makes the student discover the reasoning themselves, then checks whether it survives a case they were never taught. Adaptive guided discovery, not content delivery.
The induction method here was derived and extended from an earlier text-based prototype, Aux, an AI learning tool for medical students that teaches clinical reasoning through guided discovery rather than direct explanation. It shows students carefully chosen contrasting cases and probes them to induce the underlying pattern, with the goal of building durable illness scripts. This case study takes that method and extends it onto a holographic patient.
The problem & the opportunity
Third-year students can recite the mechanism of heart failure and still freeze at the bedside: their knowledge is inert, filed by discipline instead of by clinical cue. XR simulations render impressive patients, but a scripted scenario runs the same for everyone; it can’t adapt to how a particular student reasons. The platform owns immersion; transfer needs a tutor that responds to each learner’s thinking.
A byproduct: the reasoning becomes measurable
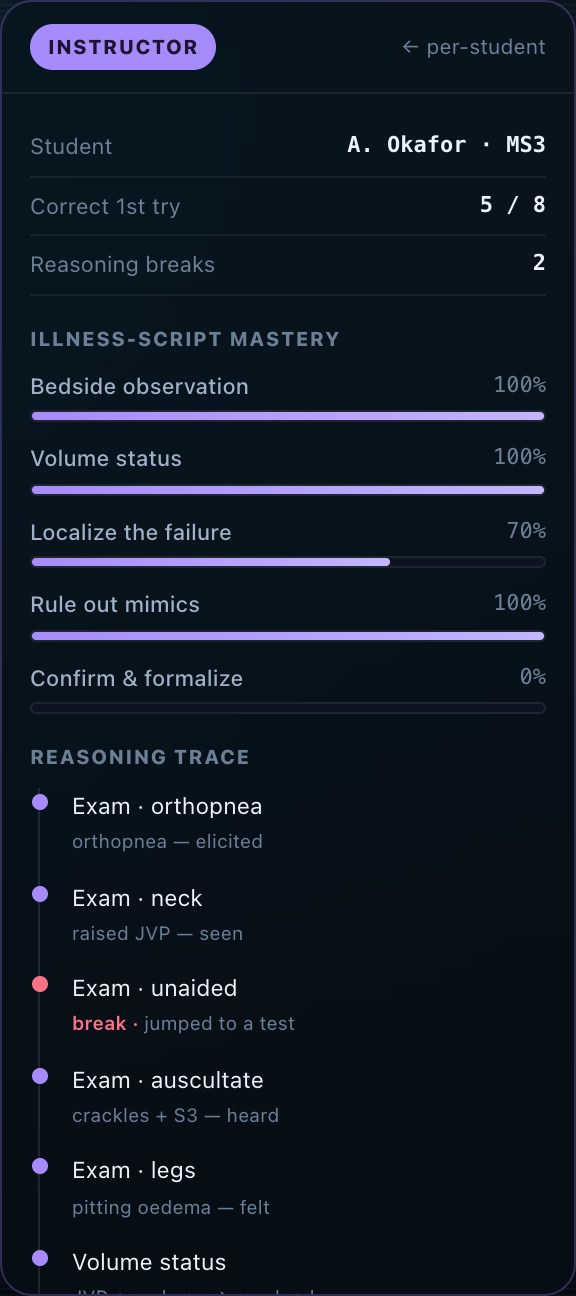
Because the student reasons in the open (free-text, step by step), the thinking is no longer hidden, and two things fall out of that. An instructor who can’t sit beside 120 learners gets a per-student read on who’s guessing, who’s pattern-matching, and who can transfer, with per-node mastery (observe → localize → discriminate → confirm) and the exact step where reasoning broke. And the method validates itself without a bolted-on exam: the signal is a transfer check, a never-taught presentation of the same illness script: did the reasoning fire on an unseen case, or only the one they practised? Both are genuine benefits, but they fall out of the method rather than drive it.
| Legs | Neck veins | Onset | |
|---|---|---|---|
| Clot in lung (PE) | one calf swollen | may rise, acutely | sudden |
| Fluid overload | both legs, symmetric | raised | over days |
Positioning: a layer, not a competitor
The sharpest decision was not to rebuild the platform. Rendering holographic patients is a solved, capital-heavy problem the XR-simulation platforms already own, and competing there burns a war chest to reach parity. So the tutor sits on top of one: it consumes the findings the patient already produces and adds the one thing a script can’t: an adaptive read on each learner’s reasoning. That turns a would-be competitor into a distribution partner and shrinks the build to “the reasoning layer.”
Scoping the MVP
Instead of “a tutor for all of medicine,” I scoped to one scenario, end to end: acute dyspnea → decompensated heart failure, chosen because its findings are visible at the bedside, exactly where attention-direction in AR earns its keep. The demo walks that full reasoning loop with the live instructor panel, so the mechanism and the outcome claim are tangible. It’s the argument for the MVP, not the shipped MVP.
Pedagogy decisions, made as product decisions
- Discovery over telling: the student induces the pattern from findings they gathered: recall, not recognition, is what transfers.
- Free-text, not multiple choice: menus give the answer away and inflate the metrics. Costlier to grade, honest about mastery.
- A fading scaffold: heavy guidance first, then the training wheels come off and it only nudges when the learner stalls; support removed as they improve is what builds independence.
Guardrails against a hallucinating tutor
In clinical education a confidently wrong answer is worse than none, so the design keeps the model out of the position to invent one. The AI never owns the clinical truth: the findings and correct illness scripts come from the validated scenario; the tutor runs the dialogue and grades reasoning against that fixed answer key, not free judgment about what’s true. When its confidence in grading a free-text step is low, it abstains and flags the exchange to the instructor, so a model slip becomes a reviewable flag, not a fact taught to a student. Validated content owns the medicine; the tutor owns the conversation.
What this is, and what’s next
This case study is an interactive demo: a representative acute-dyspnea session with the reasoning loop and a live instructor panel; it makes the method tangible, but it isn’t a shipped AR product. Next: build the layer against real holographic-patient findings, run a controlled pilot measuring transfer against slide-study, and add a second scenario to test whether the method generalizes beyond one disease.